In 1997, Congress imposed a cap on the number of Medicare-funded residency slots for medical school graduates. This had the effect of fixing the geographical distribution of funding for residency training across the United States. Government financing significantly influences where medical residents receive training, and that matters because medical residents often remain in the same area once they complete their training. Over the past 25 years, as the population of the United States has shifted, a growing disconnect has emerged between the local demand for medical services and the physician supply necessary to provide these services. These geographical disparities are one important example of the broader harms caused by continued reliance on an outdated Graduate Medical Education (GME) financing system. This system impedes competition and unfairly disadvantages primary care and rural areas. The cap on funded training slots should be eliminated as part of a broader overhaul of GME funding.
Residency location is a substantial determinant of physician practice location
Where physicians conduct their residency training greatly influences where they will wind up going into practice. Medical residents typically spend between three and seven years completing training in their chosen specialty, with many receiving additional fellowship training afterward. Over the course of this training, physicians develop significant professional, personal, and financial connections that tend to keep them in the same area when they start their own practices. The location of residency strongly influences the future practice location for all physicians, but especially for those practicing in primary care specialties. One analysis of family medicine physicians found that 56 percent ended up working within 100 miles of where they completed their residency.
“Primary care physicians are about 3.8 times more likely to pick a job within the same state of residency and about 3.4 times more likely to pick a job within the same hospital referral region as the residency. On the other hand, specialists are 2.8 times more likely to pick a job within the same state as residency and about 3.6 times more likely to pick a job within the same hospital referral region.”
Elena Falcettoni
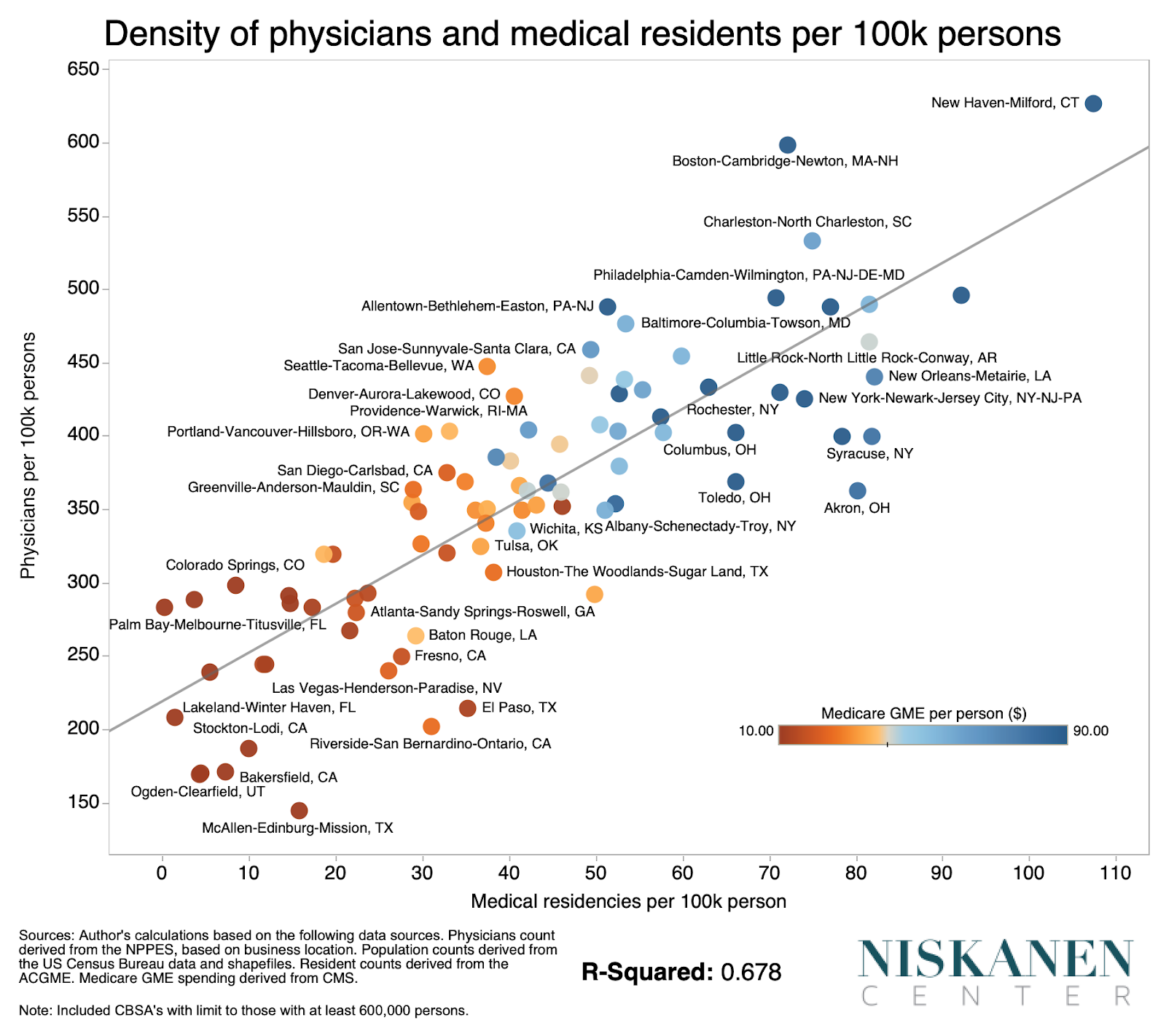
The chart below demonstrates the relationship between residency training and physician practice location across major metropolitan areas. Places that train more medical residents per person tend to have a higher concentration of physicians as well. Places such as Cleveland train a disproportionate amount of doctors per person and so have a higher concentration of doctors’ practices in the area, while the reverse is true of metros that train fewer, such as greater Atlanta or the McAllen, Texas, area.
And Medicare’s GME funding plays a huge role in determining how many residents an area can support. Not coincidentally, places that train more residents per person also receive more funding for residency training through Medicare’s GME funding streams, which is the dominant source of public funds. Given that physicians are the central providers of health care and that a growing share of Americans is reporting supply-related barriers to accessing care, policymakers should care about the disparities that stem from current policy.
The GME cap on funded slots drives geographic disparities in physician supply
We can be confident that GME funding disparities directly cause geographic disparities in medical residents’ training. In 1997, Congress froze the allocation of GME by instituting a per-institution cap on the total number of Medicare-funded residency slots. But an unintended consequence of the cap is that patterns of residency financing have remained mostly unchanged while there have been large changes in population patterns and, by extension, underlying patterns of demand for medical services.
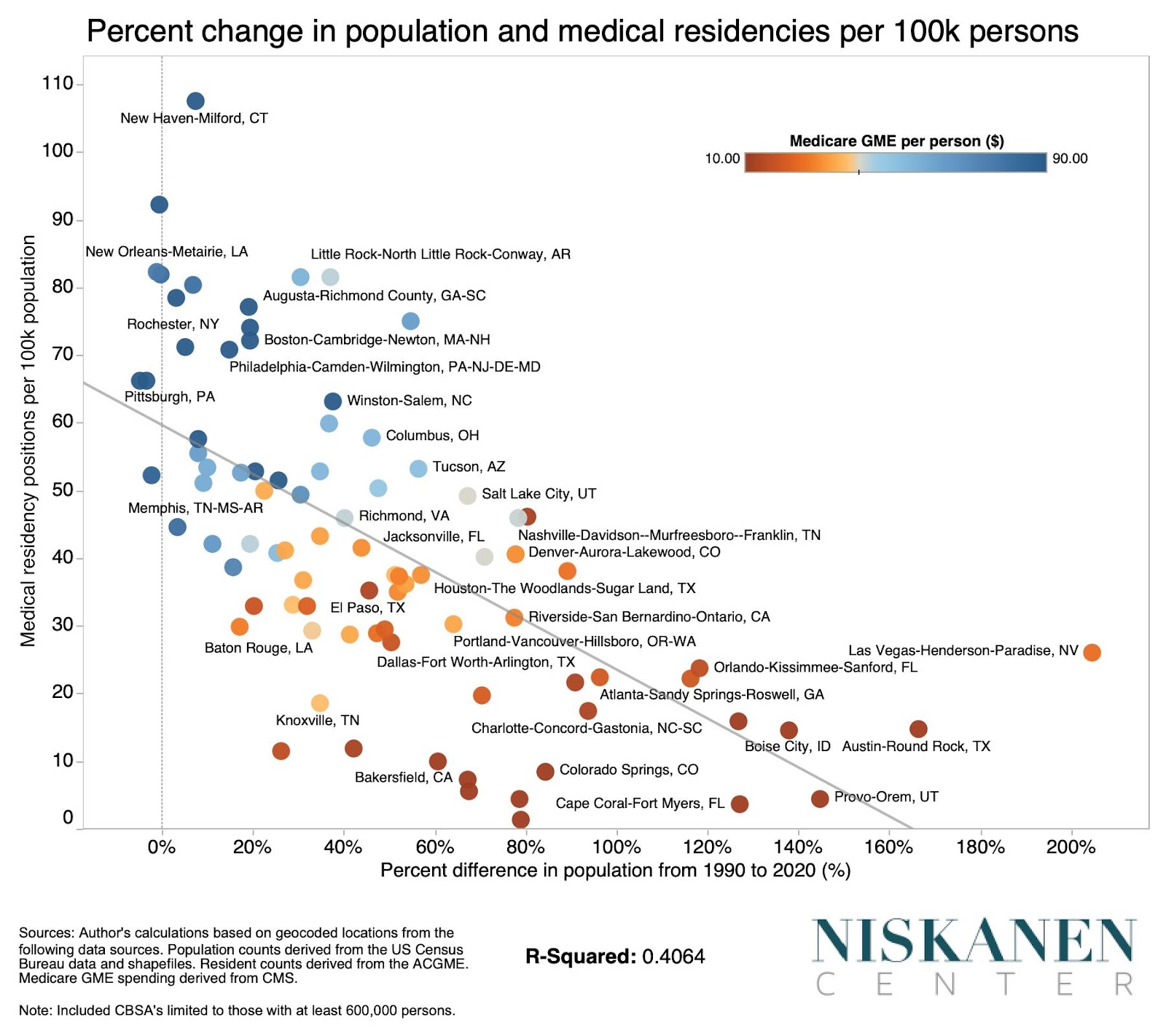
As a result, the New Orleans metro area now has one of the highest densities of medical residency training per person. New Orleans area hospitals continue to “own” the same number of residency slots as they did in 1997 even though the metro area’s population has slightly declined in the intervening 25 years. The pattern in the New Orleans metro is indicative of a broader trend, as illustrated by the relationship between residency training per person and population change since the 1990 Census.
Metros with stagnant or even declining populations, such as Baltimore, Detroit, and Pittsburgh, train a disproportionately large share of the country’s doctors, while metro areas that have grown particularly fast, such as Austin; Phoenix; Provo, Utah; and Cape Coral, Florida, train a disproportionately small share.
It is worth noting that the same pattern holds for disproportionately elderly rapid-growth communities in Florida, such as North Port-Sarasota and Deltonia-Daytona Beach. These metros are disadvantaged in the same way as disproportionately younger high-growth metros like Bakersfield, California. Thus, we can be reasonably certain that the frozen distribution of funded slots is the overriding driver of residency training disparities, rather than underlying demographic factors related to Medicare itself.
Current financing for medical residencies is anti-competitive, anti-primary care, and anti-rural
The current public funding arrangements for health care in the United States are inadequate and biased against achieving the broader physician-workforce objectives that most health care experts believe are necessary. As the largest source of financing for medical residences, Medicare shoulders much of the blame.
As shown above, the training slot cap is one major problem. The problem is not necessarily that we don’t have enough funding for residency training, but that it’s inappropriately distributed. That is because public financing for medical residency does not follow residents where they train; it is instead owned by teaching institutions themselves.
A far better approach would be to make payments mobile by eliminating the per-institution caps on funded resident training entirely. The cap was introduced as the culmination of numerous policy actions aimed taken with the goal of preventing a predicted “physician surplus.” In retrospect, it is clear that these “physician surplus” fears were unfounded. The current funding is so poorly distributed that the cap could be removed without requiring additional spending, simply by spending more wisely.
But the cap is not the only problem. The formulas that set the level of funding for residency training are badly outdated. The vast majority of this funding is delivered through the “Indirect Medical Education” (IME) program, which applies a multiplicative percentage add-on to Medicare-reimbursed services — like a restaurant tip. Because IME provides a blanket multiplier regardless of whether medical residents were pertinent to the exact Medicare services being furnished, it creates an incentive for services to be consolidated within a single large institution. Delivering funding for GME in this manner furthermore disproportionately advantages high-wage metros, magnifying existing funding boosts for these areas. The blanket multiplier approach also delivers the greatest additional dollars to facilities providing more complex procedures. The biggest losers are primary care training facilities in rural areas, where the doctor shortage is most acute.
The size of IME payments is based on the ratio of residents to hospital beds. This funding approach has become increasingly outdated as a proxy for the costs associated with training residents, particularly as the share of care delivered in outpatient settings has grown. In fact, the Medicare IME funding stream is only even available to inpatient facilities, entirely neglecting the outpatient settings where a large and growing share of care is actually delivered nowadays. That creates the anti-competitive incentive to fold ownership of these facilities into inpatient hospital networks that can capture the subsidy.
The purpose of GME financing isn’t to give handouts to lucky hospitals
The issues stemming from Medicare’s IME program are indicative of the broader problems with outdated and poorly designed funding streams for graduate medical education in the United States. Instead of implementing the structural overhauls that are needed, policymakers have either tweaked or added programs to address specific concerns, allowing the underlying problems with the system to worsen. The resulting patchwork of funding streams is both wasteful and ineffective in supporting the country’s physician-workforce needs.
The cap has proven politically durable both because lawmakers are averse to spending money in general and because some teaching hospitals make out like bandits under the current financing system. This misdirected fire hose is not only wasteful but also actively harmful to competition and the composition of the physician workforce.
Federal policy should reorganize support for residency training, consolidating the disparate GME funding streams to get more bang for our buck. Effective GME policy should aim to support the creation of the marginal residency placement where demand for medical services most exceeds the supply of service providers. A mobile relatively standardized per-resident payment would allow market forces to enter the equation.
Making payments mobile would also help to ensure greater accountability over the spending itself. Presently, public financial support for GME often gets treated like “free money” as many teaching institutions face little-to-no risk of these funds migrating to another institution. Fixing this would produce greater pressure on institutions to direct these funds toward their intended purpose: supporting the residency program.
Residency programs benefit from scale economies, meaning marginal per-resident payments should decline for teaching institutions training greater numbers of medical residents beyond a certain point. A good model along these lines is the residency financing system used in The Netherlands. The value of residents’ labor to their institutions also grows as they advance through their residency, and payments should adjust over the course of a resident’s training to reflect this.
In principle, there is no reason why overhauling GME couldn’t be done in a budget-neutral manner. That’s why it’s disappointing that so far, lawmakers have been content to throw money at a broken system. Simply adding another 1,000 slots to institutions training more residents than they are currently funded for, as recent legislation did, isn’t helpful. If additional funding is necessary to bring relevant stakeholders on board with structural reforms, it would be money well spent.
To learn more about the shortcomings of the current public financing streams, see “Unmatched: Repairing the U.S. Medical Residency Pipeline”.
Photo credit: iStock