The high cost of health care in the United States has squeezed the budgets of ordinary working Americans, increasing popular demands for the governments to pick up the tab. Yet socializing the cost of health care does little to address the underlying forces restricting supply and raising prices. On the contrary: shifting costs onto public budgets can make the situation worse, accelerating cost spirals while undermining America’s longer-term fiscal balance.
While the need to control rising health care costs and expenditures is widely recognized, there is little consensus about which reforms have the best chance of working. Fortunately, a recent working paper by Joshua Gottlieb and co-authors marks a substantial improvement in our understanding of the high share of U.S. health care spending – 9 percent – devoted to physician incomes in particular. The paper’s central question addresses how much we can realistically expect to reduce total health care spending by cutting providers’ payments.
Physician incomes are high and sensitive to government payments
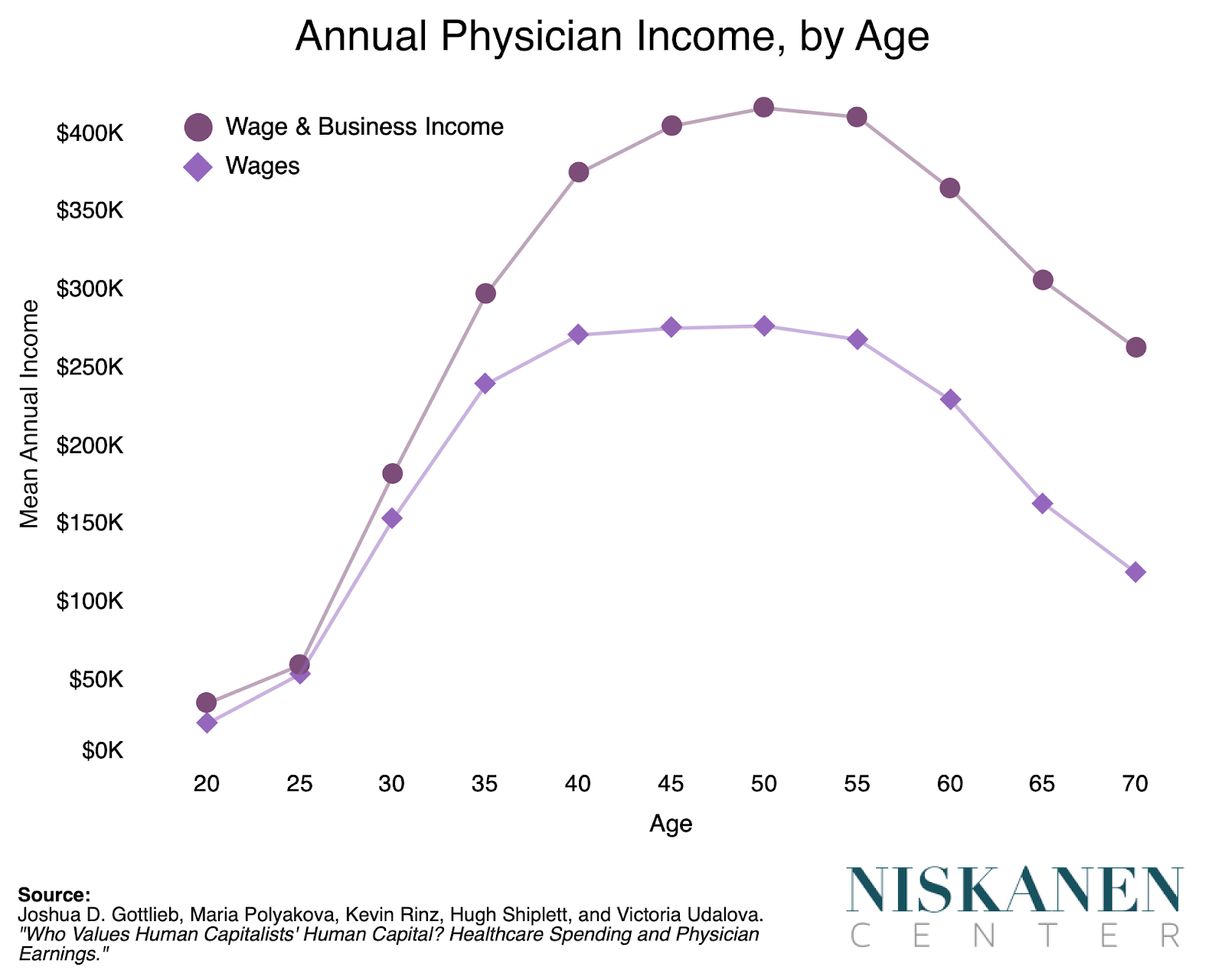
Gottlieb and his co-authors provide the most comprehensive picture of physician earnings to date, taking advantage of data linkages between IRS tax returns and other administrative data sources. In 2017, physician incomes averaged to $343,600, with the median physician earning $255,000. About 87 percent of physicians are in the top 10 percent of the income distribution, with 28 percent in the top 1 percent. The paper’s figures mark a substantial improvement over previous survey-derived estimates of physician income, which considerably underreported nonwage business incomes.
Gottlieb and his co-authors use this data to examine the impact of government payment policies on physician income. Looking at a 2013 increase in the Medicaid reimbursement rate for primary care physicians, the authors find that roughly half of this increase in payments was passed on to the physicians in the form of higher salaries. In other words, government payments can, at least in theory, substantially influence physician incomes.
Whether provider payment cuts are a practical reform option depends on how physicians respond. Cuts to physicians’ salaries could prove undesirable if fewer physicians practice medicine as a result, for example. To get at the plausibility of an adverse response, Gottlieb and his co-authors compare physicians with lawyers to get a sense of a future physician’s outside career option. This comparison between physicians and lawyers is meaningful due to several similarities between the professions, including state-level licensure requirements, as well as both requiring substantial personal investments in education and training.
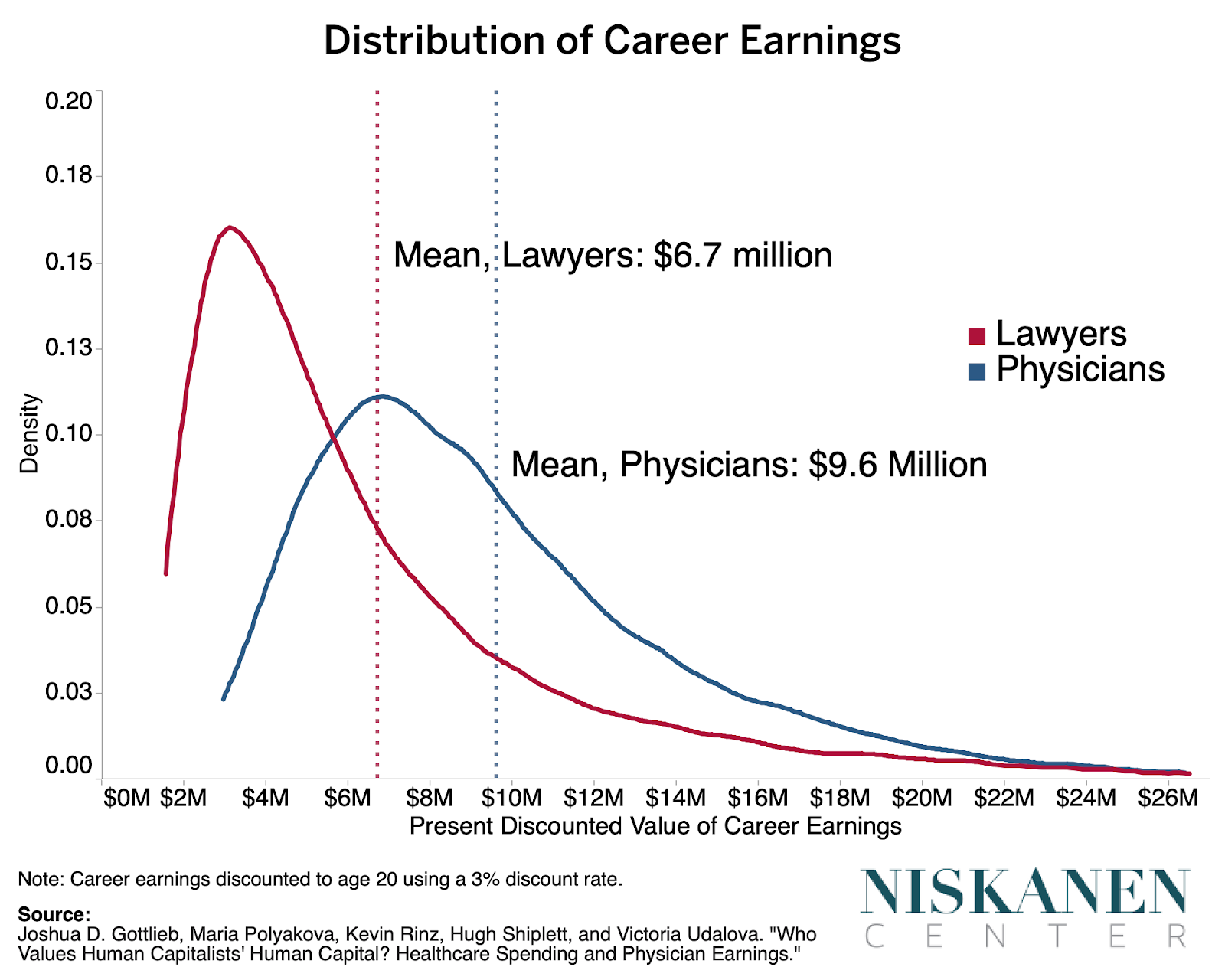
To compare the relative attractiveness of physicians with lawyers, Gottlieb and his co-authors look at the distribution of lifetime earnings across both careers. To account for differences in education and training, earnings are calculated based on their present discounted value at age 20. Discounting reflects the sensible intuition that a dollar earned today more valuable a dollar earned in the distant future. This is important to account for, since physicians typically enter the workforce at a later age than lawyers and experience substantially reduced earnings during residency training.
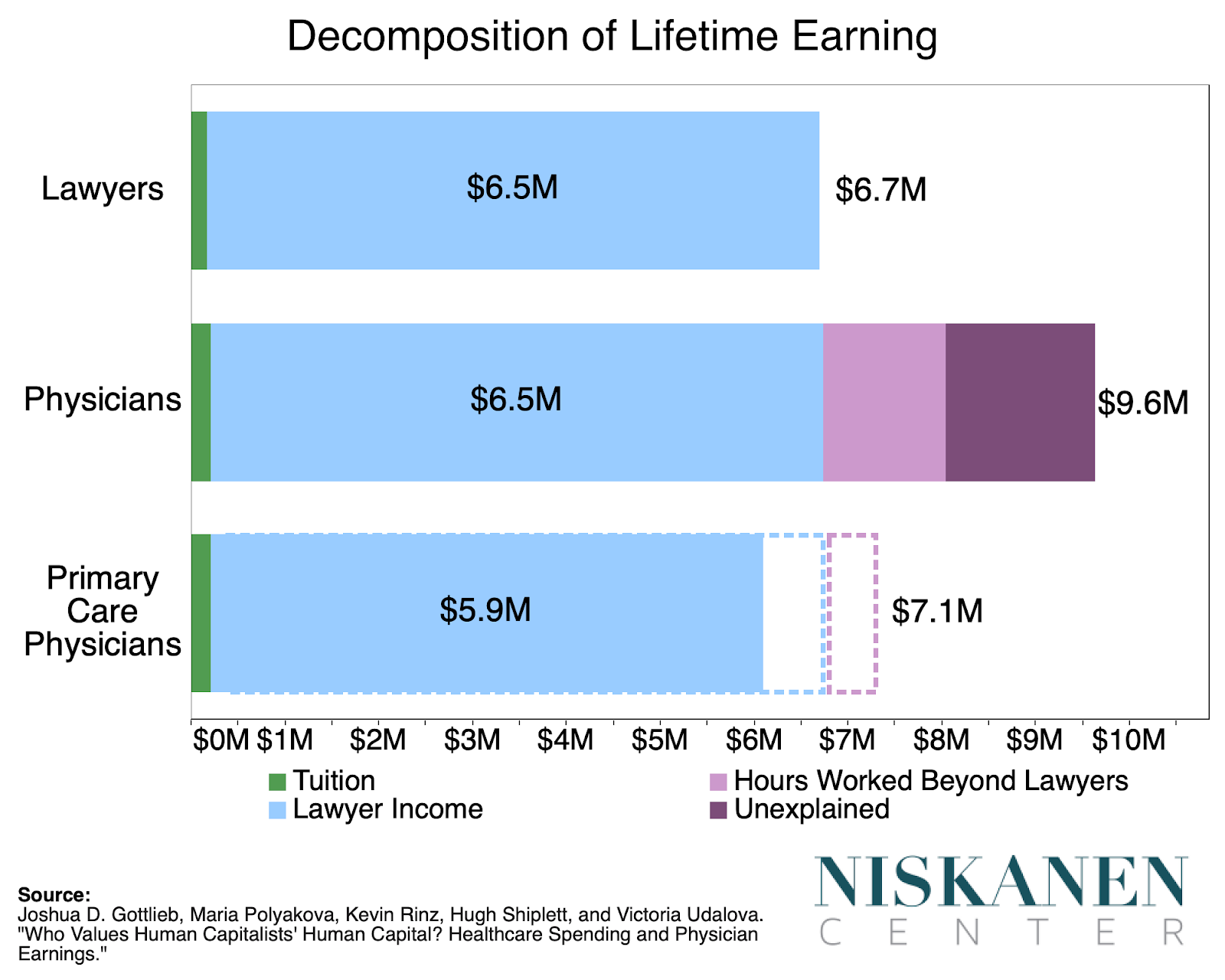
While both career paths are subject to a great deal of variation, physicians earn about 40 percent more than lawyers over a career. After accounting for physicians’ higher training costs and longer working hours, average physician income is about 25 percent greater than that for lawyers.
Crucially, however, expected lifetime earnings among primary care physicians (PCPs) are actually lower than those of lawyers. Taking into account primary care’s longer working hours further worsens its relative financial attractiveness compared to law. The authors’ definition of PCP includes specialties such as family and internal medicine, and includes 44 percent of all U.S. physicians.
So while physicians on the whole are quite well-compensated, primary care physicians are much less so. And from the standpoint of enacting cuts to provider payments, relatively unattractive PCP compensation is potentially problematic. The danger here is that prospective primary care physicians might instead opt to pursue specialties outside of primary care, or even a career outside of medicine altogether.
Compensation of non-primary care specialties is excessive relative to labor market fundamentals
Non-primary care (NPC) specialists make up about 56 percent of all physicians and experience significantly higher levels of compensation.
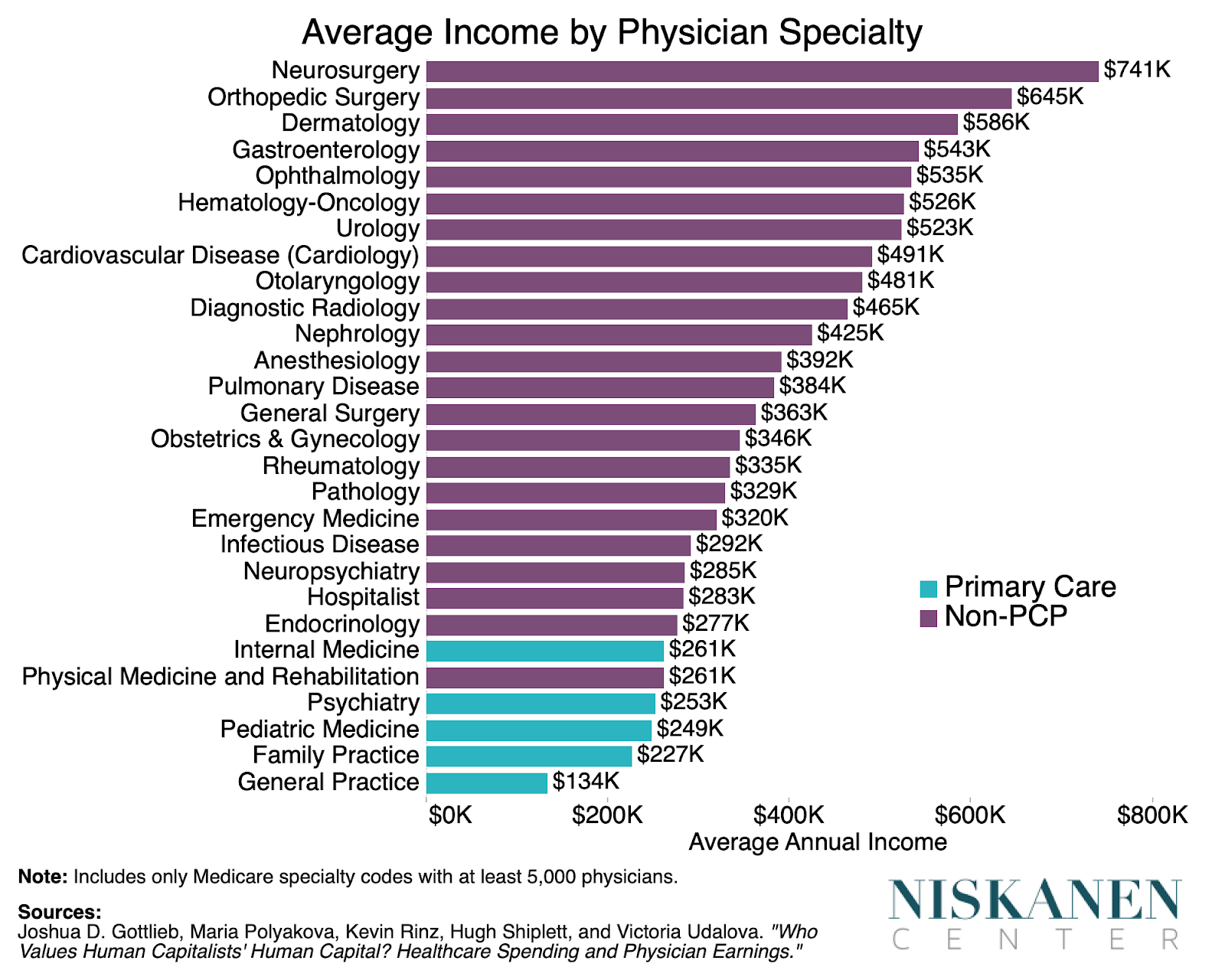
Part of the income premium experienced by NPC specialists reflects labor market fundamentals. For instance, the most highly paid specialties tend to work more hours per week and train for more years during residency. But such fundamentals alone cannot plausibly explain the exceptionally high earnings of NPC specialists.
Looking at physician pay from an international perspective confirms the importance of NPC specialties when considering any hypothetical cuts to physician payments. While American physicians earn far more in dollar terms than their European counterparts, Gottlieb and his co-authors find that the U.S. is far less exceptional when looked at in terms of doctors’ relative position in their respective countries’ income distributions. U.S. primary care physicians are in the top 1 percent of our income distribution with similar frequency as Swedish or German physicians are as a whole. This suggests that any conceivable realignment of U.S. physician compensation would need to primarily target the extraordinarily high pay of NPC specialists.
Physician incomes are higher where they are less numerous
Another distinctive characteristic of physicians’ incomes is their departure from high-productivity professions’ tendency to have higher incomes in denser, more productive regions. The highest average physician incomes are instead found in more sparsely populated states.
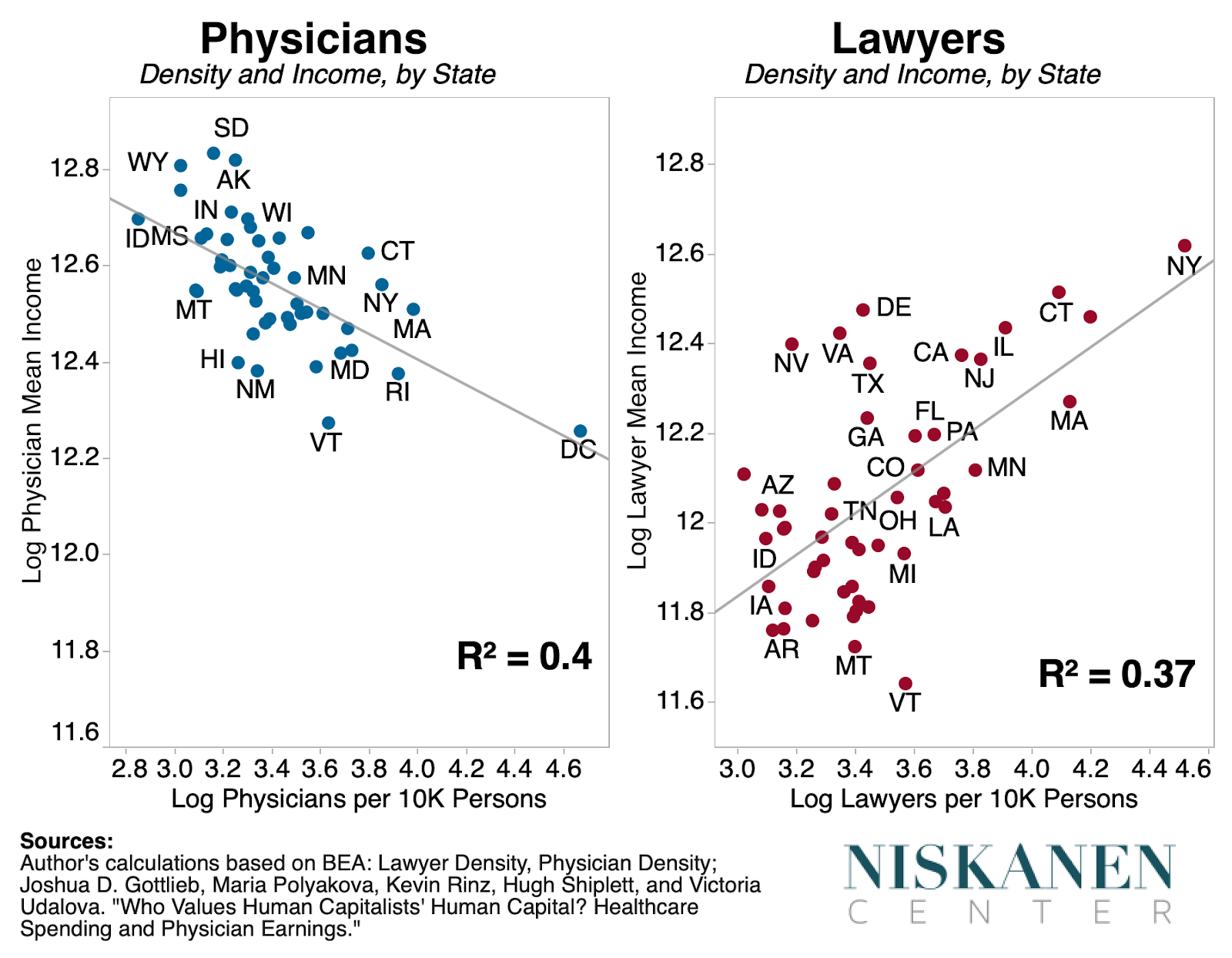
Unlike many high-skill professions, physician services typically require in-person delivery, often on short notice. As such, geographic proximity is highly determinant of whether a physician can meet a given patient’s needs. By contrast, proximity is much less important for professions involved in the production of tradable goods and services. Lawyers cluster in New York City, for instance, but readily provide their services to clients across state, and even national, borders through the use of communication and information technology. We might expect, therefore, that fewer physicians per person in a given area would grant such physicians greater pricing power.
The inverse relationship between physician income and physician density is significant because there are substantial economic pressures running in the opposite direction, including the productivity-enhancing effects of cities, Baumol’s cost disease, and health care’s properties as a “luxury good.” We should therefore expect that taking the ratio of physician incomes with regional differences in personal consumption per capita would strengthen the inverse relationship between physician income and density, while weakening the positive relationship between lawyers and density. And that’s exactly what we observe.
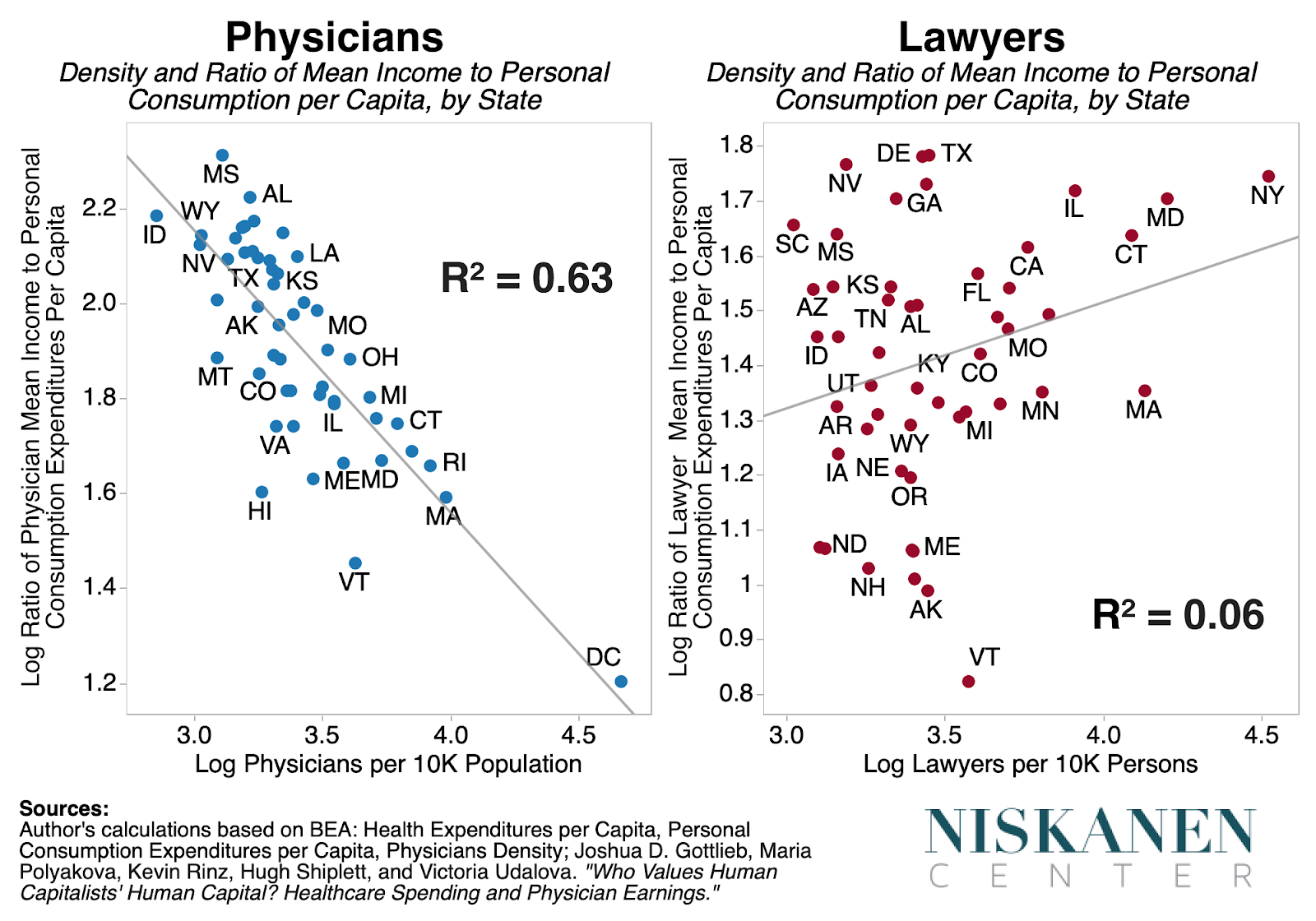
Analyses by Gottlieb and his co-authors back this up, finding that physicians operating in areas with lower levels of competition as measured by the Herfindahl-Hirschman Index have higher incomes, even after controlling for a variety of physician characteristics including age and specialty.
Though rural physicians’ incomes do tend to be higher, cutting payments to these providers isn’t necessarily a slam dunk. The higher earnings experienced by physicians in lower density settings may, at least in part, reflect the premium necessary to compensate for forgone urban amenities. Care ought to be taken to ensure that cuts to provider payments don’t disproportionately harm areas already dealing with a shortage of health providers.
The decision of whether or not to cut provider payments would be more straightforward if the United States had more physicians in the first place. Instead, the United States currently has far fewer physicians per person than its European peers. Since physician services are not easily tradeable, a low-density country like the U.S. needs to have significantly more physicians than the rich E.U. countries to get the same level of accessibility.
Implications for health care policy
Gottlieb and co-authors have done a tremendous job of not only in putting together the richest portrait of physician incomes to date, but also in providing useful comparisons from which to draw a number of conclusions for health care policy:
- Indiscriminate cuts to physician providers could backfire:
In terms of compensation, a career as a primary care physician is relatively unattractive compared with the alternatives available to medical students. The per capita supply of primary care physicians in the U.S. has already deteriorated in recent decades. This is worrying because PCPs provide crucial front-line care, and their density is more strongly associated with public health metrics than that of non-PCP specialists. Further squeezing these providers’ incomes could thus worsen public health outcomes, particularly in rural areas and underserved communities.
“Medicare for All” is a recent example of legislation that would, if enacted, impose provider cuts in an unfocused and indiscriminate manner. As currently drafted, all provider compensation would be moved to Medicare rates, which are lower than those of private insurance. If “Medicare for All” or legislation with similar impacts on provider payments were ever to be seriously considered, its effects on the distribution of physicians by specialty and geography would demand careful study, and possibly need to be revisited in favor of more targeted cuts.
- The most viable payment cuts are targeted at non-PCP specialties:
Previous studies have pointed to barriers to entry as the likely culprit behind excessive incomes for some specialties. Residency Review Committees (RRCs) governed by members of the specialty in question exert total control over the number of residents trained within each specialty. RRCs can thus easily create rents for members of their specialty by limiting competition. And to the extent that the income premium provided to NPC specialists genuinely reflects such rents, there’s a good case for targeted cuts to their provider payments. In particular, Gottlieb and his co-authors identify radiology, ophthalmology, anesthesiology, and dermatology as specialties where incomes depart most substantially from underlying labor market fundamentals.
The role of specialties in driving excessive salaries is brought into sharp relief when looked at internationally. Specialties not only command a greater earnings premium in the United States but also make up a significantly larger share of the physician workforce. Even primary care roles in the U.S. are more likely to be performed by individuals trained in a specialty, such as internal medicine or family practice.
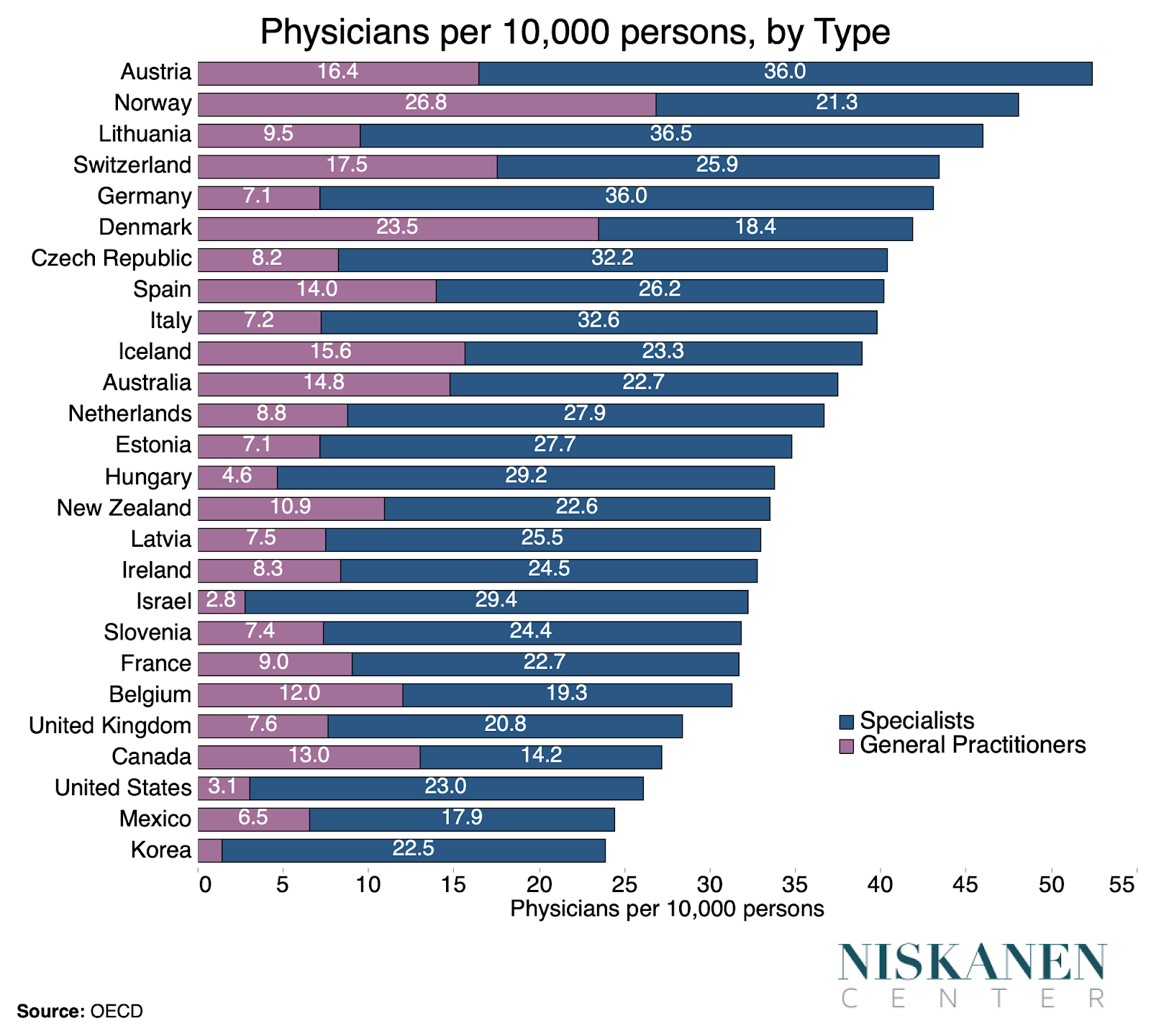
The tendency towards increasing specialization shows no signs of abating, with more and more physicians not only pursuing specialties but, increasingly, sub-specialties as well. For comparison, neighboring Canada has four times as many general practitioners per person despite having a similar number of physicians per person. Like the United States, Canada embarked on a quixotic campaign to constrain its physician numbers due to fears of a “physician surplus” that never arrived. Unlike the United States, however, Canadian provinces take an active role in diverting resources to primary care, particularly since the early 2000s. Consequently, the Canadian income gap between generalist and specialty care is significantly smaller, resulting in far more Canadians practicing primary care instead of more lucrative specialties.
All this isn’t to claim that we have too many total specialists. The bulk of studies does seem to imply that specialists provide superior performance regarding discrete medical procedures compared with generalists. So while it would be ideal to have more of both specialists and generalists, until that point there’s a strong case for incentivizing more of our limited physician workforce to practice primary care, at least on the margin, in order to expand access to basic health care. The evidence suggests that America would see superior public health outcomes as a result.
- The public benefits of “free medical education” are likely limited:
Zeroing out the cost of education for medical enrollees would likely have a limited impact on salaries or specialty mix. Though physicians spend, on average, about $220,000 between their bachelor’s and medical school degrees, the impact on their finances is quite small when viewed in terms of the present discounted value of career earnings. Gottlieb and his co-author conclude that this implies we should not expect making medical school education less expensive or free to have a substantial impact on specialty choice or create significant space to cut payments to physicians.
- Shortening medical education could curb health spending without adversely impacting physician incomes:
Bringing U.S. medical education in line with international standards is one way to increase physician lifetime earnings while simultaneously increasing the feasibility of cuts to government payments. While prospective physicians in most countries begin a 6-year medical degree following the completion of high school, the United States is among a handful of countries in the world where a 4-year bachelor’s degree is requisite for entry into a 4-year medical school program. The U.S. medical education system not only makes medical education a more expensive investment than it would be otherwise but also robs physicians of two years of career earnings and shifts peak-earnings years to later in life. Using the present discounted value framework employed by Gottlieb and his co-authors to assess lifetime earnings is illustrative here. Under plausible assumptions, adopting a six-year medical education track would close the lifetime earnings gap between PCPs and lawyers.
- Wither the primary care physician?
An alternative to shoring up the finances of primary care physicians is gradually abandoning them altogether in favor of nurse practitioners and physician assistants. It may simply be that the numerous barriers to entry, extended medical education, restrictive residency review committees, and the like are too politically difficult to fix. Instead, the United States may be forced to develop a health system that treats non-physician providers as the front-line of care in order to achieve the level of access to basic care found in other rich countries. In certain respects, the amount of training and education required for PAs and NPs in the U.S. is more suited to primary care practice than the extremely specialized education we require of physicians.
- Lowering barriers to interstate trade in medical services could help ease geographic disparities:
Areas with lower physician density and market concentration are associated with higher physician incomes. While targeting cuts at physicians in areas where they are less plentiful could be counterproductive, prompting physicians to leave underserved areas entirely, there is much we can do to streamline cross-state trade in medical services. Adopting a nationwide medical license and removing barriers to telemedicine would be good places to start.
Conclusion
I have touched on a tiny sample of the health policy areas that could be informed by Gottlieb and his co-authors’ findings. While cutting physician provider payments may be a viable option, this route is not without risks. Many of the tradeoffs involved in deciding whether or not to cut provider payments would become easier if the United States had more health care providers in the first place. In areas ranging from attending medical school to matching with residencies, the United States makes practicing medicine more difficult than other countries. Fortunately, from the standpoint of public policy, this leaves a lot of low-hanging fruit ripe for reform.
Robert Orr is a poverty and welfare policy associate at the Niskanen Center.
This commentary is part of our Captured Economy of Cost Disease series exploring the role of regressive regulation in driving-up the costs of core goods like health care, education, and housing. It is made possible thanks to the generous support of the Peter G. Peterson Foundation.