Occupational licensing, or state-approval to work in a given profession, is a pervasive feature of the health care sector. All told, about 14.3 million U.S. health care workers are subject to licensing, accounting for 28.33 percent of the entire licensed workforce. A growing body of research links licensing to adverse consequences, including lower employment within licensed professions and higher prices charged to consumers
Given the costs associated with occupational licensing, it is worth investigating how the relative stringency of health care licensing in the U.S. compares with that of other high-quality health systems abroad. Compared to other wealthy European countries, three major differences stand out:
- The scope of licensure in the U.S. is broader, encompassing more entry- and mid-level health care workers.
- U.S. licensing processes contain more onerous requirements in the form of fees, paperwork, and other administrative hurdles.
- Work authorizations granted by U.S. licenses are generally limited by state boundaries, resulting in barriers to employment and innovation not found in Europe.
Putting all of this together, health care occupational licensing in the United States is more pervasive, burdensome, and restrictive compared to our European counterparts. Reforming occupational licensing within health care is therefore of the utmost importance for making the broader U.S. labor market more dynamic. This is all the more true amid the COVID-19 epidemic, as restrictions created by excess licensure and related administrative burdens impede the public health response.
More Pervasive
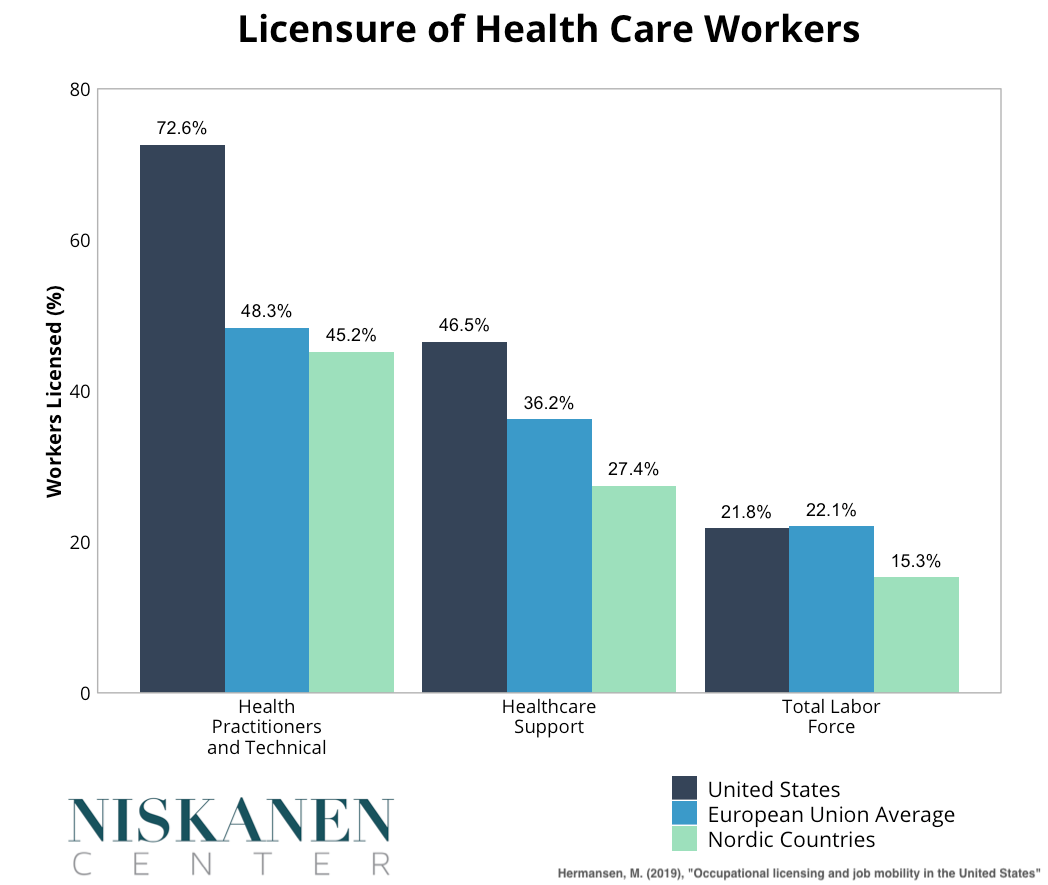
Licensure requirements in the United States cover a broader swath of the health care workforce than in Europe, even though a similar share of the overall medical workforce is licensed on both sides of the Atlantic. Within Europe, the lowest licensure rates are found in Nordic countries such as Sweden, Norway, and Denmark.
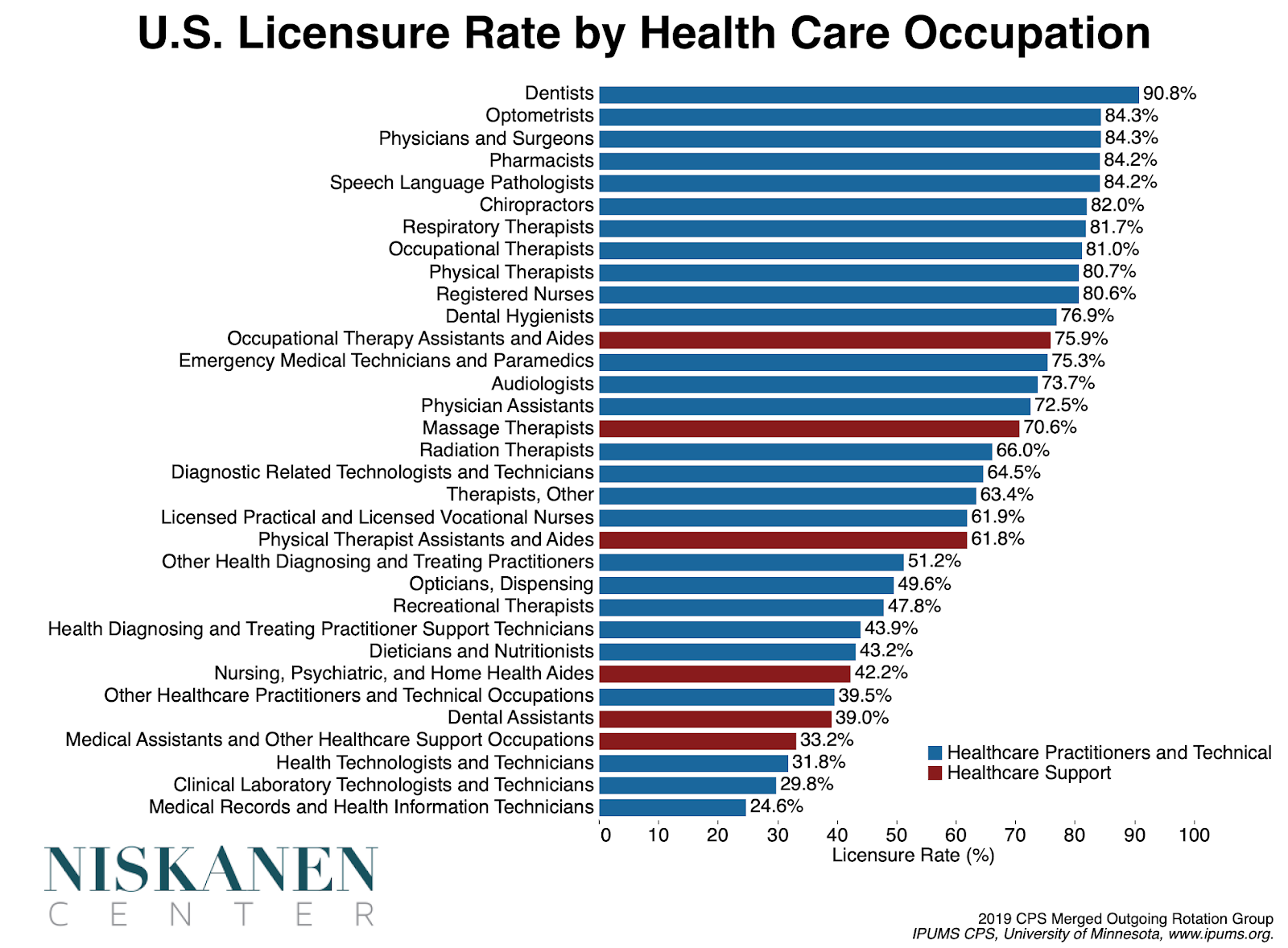
Looking at data from the Current Population Survey helps break down the picture of licensure in the United States further. Every European country and U.S. state licenses medical doctors. The only physicians who aren’t licensed are either in the pre-licensure stage of the profession or else working in a role that does not directly interface with patients. What sets the United States apart from many of its European peers is the range of health care workers who are subject to licensure.
European countries exhibit a significant degree of variation in the occupations they license. While Denmark has the lowest overall rate of occupational licensure in Europe, it still licenses some occupations that remain unlicensed elsewhere. For example, dispensing opticians, responsible for fitting eyeglasses and contacts, are licensed in Denmark but are unlicensed in other European countries as well as some U.S. states. Still, comparing how often licenses are required across countries reveals some broad trends regarding which occupations are more and less likely to be licensed.
Comparing required licenses in the United States with required licenses in the least licensed European countries, such as the United Kingdom, Sweden, and Denmark, highlights two broad areas in which the U.S. licenses more on a systematic basis.
1. Junior-level and supporting health care roles.
Licensure requirements for U.S. health care workers encompass more occupations that perform junior-level support duties. These positions often have the title of “aide,” “assistant,” or “technician.” To illustrate, while most European countries license physical therapists, U.S. states often require licensure of physical therapy assistants and aides as well. The duties performed by these professions often include hands-on patient care as well as diagnostic tests, keeping patient records, or maintaining equipment.
For example, the professions of health care assistants and physician assistants (PA) are unlicensed in the U.K., while their counterparts in the U. S are licensed. Even nursing assistants, the quintessential entry-level health worker, must be licensed by American state boards. The entry-level and mid-level health providers that form the backbone of the U.S. health system face administrative burdens and regular fees that their European counterparts typically avoid.
2. Therapeutic forms of care where the risk of harm is negligible.
The second grouping of occupations where the United States licenses to a greater extent is health professions engaged in delivering low-risk forms of therapeutic care. The professions in this grouping include speech-language pathology and various forms of therapy, such as massage therapy, art therapy, and music therapy. These occupations are licensed in either some or all U.S. states but remain largely unregulated in European countries with low rates of licensure.
More Expensive
The United States not only licenses a large share of its health care workforce, but the licensure process for these workers is also unusually burdensome. Unlike in most countries, health worker licenses are not valid throughout the whole country. Instead, the right to provide health services is determined on a state-by-state basis, though some states have signed onto compacts that ease the burdens here to varying degrees.
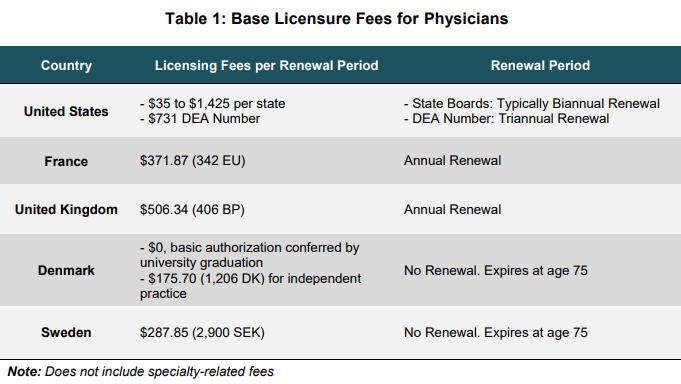
Over the course of a career, many U.S. physicians end up paying fees totaling tens of thousands of dollars. For physicians, state medical boards vary significantly in the application fees that they charge for licensure, ranging from $35 in Pennsylvania to $1,425 in Nevada.[1] In addition, all prescribing physicians must pay $731 every three years to the Drug Enforcement Administration. Relative to what is typical in Europe, overall fees for a physician licensed in a single U.S. state range from slightly lower or substantially higher. Compared to Nordic countries, licensing costs in the cheapest U.S. state are exponentially higher over the course of a career.
For physicians licensed in multiple states, licensure-related fees are almost certainly higher than any found in Europe. Unlike the U.S., almost all European countries license health professions at a national level. As a result, the need to purchase multiple licenses to practice health care is a burden that is largely unique to the U.S. Currently, over 22 percent of physicians are licensed in at least two U.S. states, and 7 percent of physicians maintain licenses in 3 or more states. To achieve physician licensure throughout the entire U.S. would cost well over $10,000 in renewal fees every couple of year. Only 14 doctors in the entire country are licensed in all 50 states.
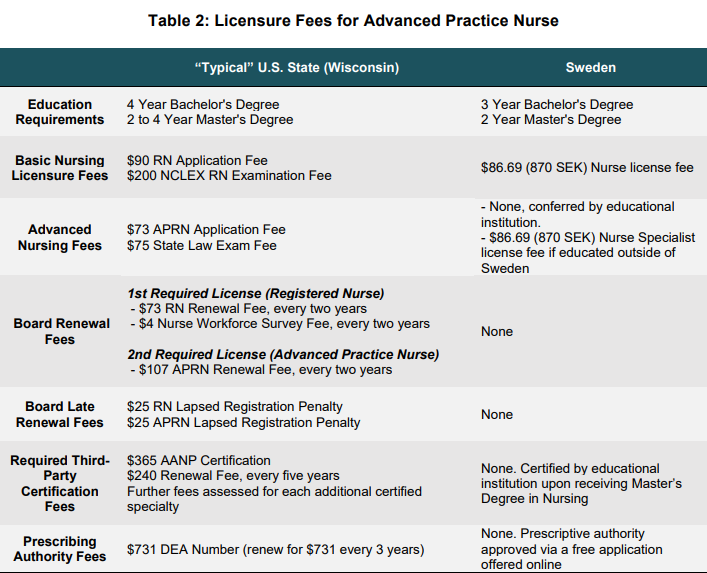
Nonphysician health occupations often face even greater hurdles in the United States. Advanced practice nursing (APN) provides an illustrative point of contrast between the highly burdensome health worker licensing system in the United States and the streamlined processes used in Scandinavia. The United States and Sweden are both at the forefront of reforms to expand scope of practice for nurses, allowing nurses with a Master’s Degree to perform many of the medical tasks traditionally reserved for physicians. However, the two have taken very different regulatory paths to the budding profession.
The cost of a nursing license is 870 Swedish Krona, or about $86.69. For nurses educated at a Swedish university, this amounts to a single one-time payment for all nursing occupations, including advanced practice nurses. Advanced nurses educated outside Sweden must pay an additional 870 Swedish Krona for a nurse specialist license. By contrast, the United States requires multiple layers of licensure from the state board, certification from a non-profit professional association, and regular fees for federal approval of prescriptive privileges.
Over the course of a career, advanced practice nurses in the United States can expect to pay well over $15,000 in licensure-related fees. Whereas in Sweden, advanced nurses face nominal fees and certification is granted along with the degree. Each state also imposes its own unique requirements, such as Wisconsin’s requirement that advanced nurses pay for and pass a state law exam. And this isn’t even accounting for the fact that the United States keeps them in school and out of the workforce longer while loading them up with graduate-school debt whose terms are far less favorable than those for a Bachelor’s Degree.
The administrative and paperwork burdens facing health care workers in the United States are in a class of their own. Licensure processes are substantially more streamlined in Europe, requiring only basic documentation such as identifying information and proof of education or certifications. U.S. states typically require much more documentation. State-specific law exams, lengthy applications containing multiple notarized documents, multiple character references, additional certifications, criminal background checks, and an in-person interview with the licensing board are just a handful of special requirements that states impose on health care licensure applicants. Excessive administrative burdens are not merely the domain of physicians, but extend far down the chain of medical authority. For example, Maryland, Oklahoma, Louisiana, Minnesota, and Maine require dental hygienist applicants to sit down for an interview with the board as a condition for licensure.
Administrative burdens are only magnified by the state-by-state patchwork of health care licensing authorities. Health professionals who move or want to practice across state boundaries not only must undergo an additional round of licensure, but typically must also provide additional documentation from each board they were previously licensed under, with additional fees assessed by both the new and previous boards.
More Restrictive
The combination of licensure being both more pervasive and more burdensome in the United States results in the practice being far more restrictive than in other countries.
A recent report from the OECD analyzed the impact of occupational licensure across industries in the United States, finding harmful effects along a number of dimensions. The study accounted for both the pervasiveness of licensing and the heterogeneity across states and occupations. Licensure was associated with fewer transitions out of joblessness, particularly for those with a criminal record, as well as less job-switching between employers.
The barriers that licensing creates on re-employment are particularly troublesome. Unlike in most European countries, U.S. states often license even entry-level occupations such as nursing assistant. For individuals facing precarious financial circumstances, the requisite fees and time spent in mandated courses, studying for and taking exams, and waiting on paperwork to be approved may not be worth the potential financial gain from moving into the health care sector in the first place. The situation is even bleaker for America’s roughly 20 million felons, who are generally ineligible to work in the health care sector as a consequence of state boards requiring a spotless criminal record. With health care jobs accounting for more than 12 percent of employment — a share that is only set to grow further — the burdensomeness and pervasiveness of U.S. health licensure represents a significant cost for the entire U.S. economy.
The lower rate of job-switching is another cause for concern regarding U.S. health care licensure. Movement between different employers is associated not only with productivity gains for the industry, but upward economic mobility for individuals as well as higher rates of employment within an industry. Yet the layers of red tape imposed by state boards often make job switching exceedingly difficult in the U.S. relative to Europe.
**A 2019 Arizona law ensures expedited licensure approval for all health care professions.
Not only do U.S. licensing requirements reach down to entry-level professions, but the scope of the licensed occupation is also more highly specified. For instance, Maryland’s board of nursing specifies two levels of nursing assistant roles: certified nursing assistants (CNA) and geriatric nursing assistants (GNA). While many European countries don’t even license these positions, previously licensed CNAs in Maryland must pay for and complete two additional exams in order to receive their GNA license. Highly granular specification of professional licensing in the United States constrains the pool of eligible hires for different positions by placing breaks on career development within the field.
Cross-state job-switching is even more difficult. Health workers’ authorization to work in their licensed occupation typically ends at the state’s borders. Moving to a position in another state requires paying fees, filling out extensive paperwork, and possibly meeting numerous other burdensome requirements, including exams or an interview with the state board.
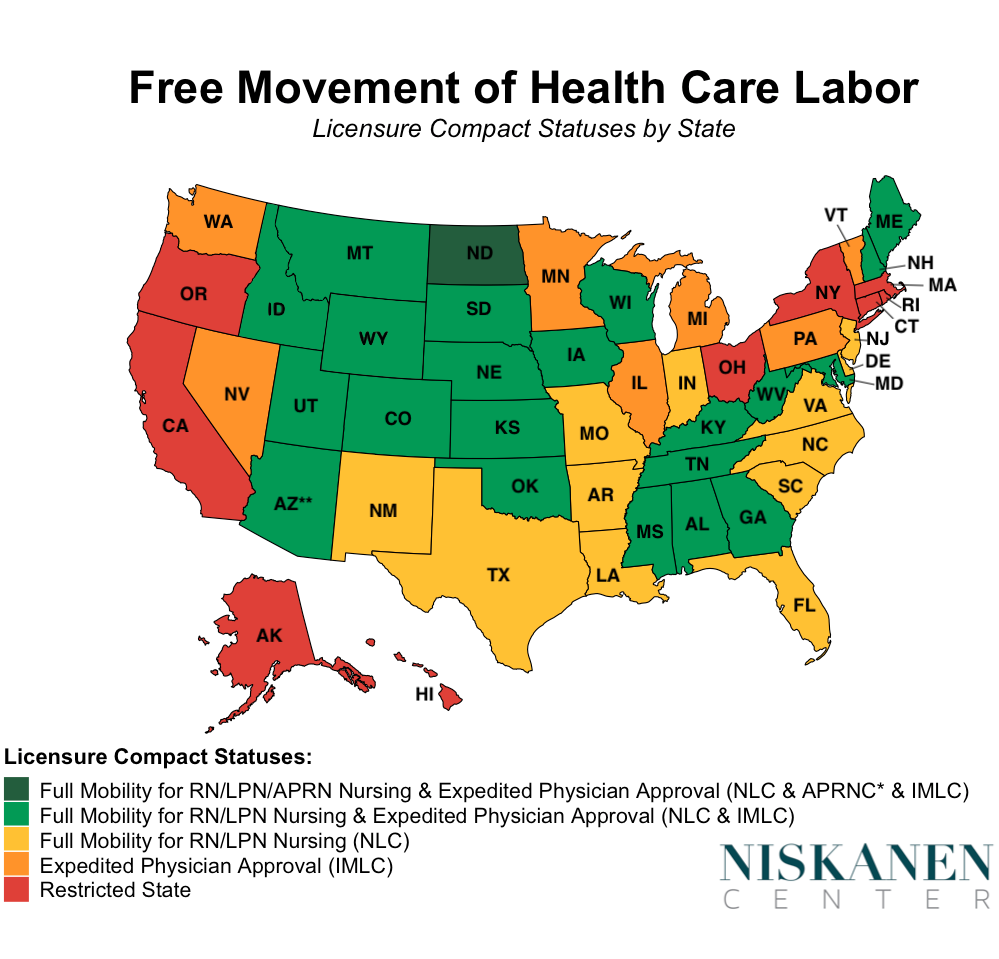
State efforts to promote mutual recognition of health care workers licensed in other states have so far stopped short of the nationwide work authorizations that Europeans enjoy. A number of interstate compacts aim to ameliorate these licensing barriers to a certain extent, including the Interstate Medical Licensure Compact (IMLC), the Nurse Licensure Compact (NLC), and the Advanced Practice Nurse Compact (APRNC). However, all of these compacts are limited by incomplete adoption by states. Additionally, the IMLC doesn’t ensure full portability, but rather provides a streamlined process that nonetheless leaves physicians responsible for all the fees assessed by each state. Compacts also operate in a patchwork fashion for some other professions, including physical therapists, psychologists, and emergency medical technicians. Many other health care professions, such as physician assistants, lack any interstate measures to ease cross-state licensure whatsoever.
The fractured state of health care work authorization doesn’t merely cause difficulties for workers who change residence, but can be a barrier to signing on with an employer just a few miles away. There are fifteen U.S. metropolitan areas with populations over one million that cut across state lines. The Philadelphia metropolitan region actually spans 4 separate states. Health workers in these metro areas, as well as countless smaller border communities, face licensing-related administrative obstacles to switching employers that would be unthinkable almost anywhere else in the developed world.
Finally, U.S. licensing rules create substantial barriers to the emerging field of telemedicine. Regionalized licensing in the United States prevents the promise of location-blind medical care from reaching its full potential. The increased hassle and expense of multistate licensure deters telemedicine providers from offering nationwide services. European countries that license nationwide do not face comparable difficulties. Even Germany, which is the most heavily licensed country in Europe and requires local membership in a health provider association, does not have such extreme barriers to nationally comprehensive telemedicine. This is because Germany’s location-based licensure requirements are tied to residence rather than area of practice.
One surprising bright spot for U.S. health care licensing is the Department of Veterans Affairs (VA). Employees of the VA enjoy exemptions from many state licensing restrictions. In order to work for VA facilities, physicians, nurses, and other health professionals need merely to be licensed in any one of the 50 states. Since the VA is not beholden to the interests of state licensing boards, it can use its federal authority to bypass state-level restrictions that run contrary to ensuring patient access. A Government Accountability Office report found that imposing state-by-state licensing on the VA would likely result in tangible difficulties with hiring and telemedicine operations, while producing no discernible benefit.
Conclusion
Health care licensing in the U.S. is more pervasive, burdensome, and harmful than elsewhere. Nordic countries like Sweden and Denmark offer a useful benchmark for reforming licensing regulations. The United States should license professions more selectively and attempt to streamline processes as much as possible. Federal measures to enact nationwide licenses or encourage states to mutually recognize out-of-state licenses should be strongly considered. The significance of this issue to broader societal concerns such as rising health care costs has likely been underemphasized. Occupational licensing reformers should place a greater focus on health care going forward.
Robert Orr is a poverty and welfare policy associate at the Niskanen Center. His research focuses on welfare, health care, and economic development.
[1] While the initial licensure in Pennsylvania is exceptionally cheap, renewal fees rise to $350 every two years. This is still below the national average.